15 Green Lane East, Remuera, Auckland, New Zealand
Monday - Friday: 7:45 am - 5:00 pm
Basal cell carcinoma (BCC) is the most common type of skin cancer in New Zealand, accounting for around 80% of all non-melanoma skin cancers. While often slow-growing, BCC can be locally invasive and cause significant tissue damage if left untreated. Mohs micrographic surgery is the gold-standard treatment for achieving complete tumour clearance, as it allows precise, layer-by-layer removal and immediate microscopic examination to ensure all cancer cells are eliminated while sparing as much healthy tissue as possible.
Basal cell carcinoma (BCC) is a type of non-melanoma skin cancer that arises from basal cells located in the deepest layer of the epidermis. It is the most frequently diagnosed skin cancer in New Zealand, particularly in individuals with fair skin and a history of cumulative sun exposure.
BCC typically develops in areas of the body that receive the most ultraviolet (UV) radiation — such as the face, neck, scalp, and hands — but it can occur anywhere. The cancer tends to grow slowly and rarely spreads to other organs; however, it can become locally invasive and cause significant tissue destruction if left untreated. While BCC is not usually life-threatening, early diagnosis and treatment are important to prevent cosmetic and functional complications

Basal cell carcinoma is the most common type of skin cancer. It develops in the basal cells, which sit in the deepest part of the epidermis (the outer layer of skin). BCC usually grows slowly and is highly treatable, especially when found early.
Even though it rarely spreads elsewhere in the body, it can still cause problems if it’s left untreated. Over time, it can grow wider and deeper, affecting surrounding skin and nearby structures. This is why doctors recommend assessing and treating it rather than “watching it” indefinitely—early treatment is usually simpler, with a smaller procedure and a better cosmetic outcome.
BCC is most commonly caused by long-term exposure to ultraviolet (UV) radiation—mainly from the sun, and sometimes from tanning beds. UV can damage the DNA in skin cells. When that damage builds up over time, it can trigger cells to grow in an uncontrolled way.
You may be at higher risk if you:
It’s also common for BCC to appear in sun-exposed areas such as the face, ears, scalp, neck, shoulders, and upper back—but it can occur anywhere, including less-exposed areas.
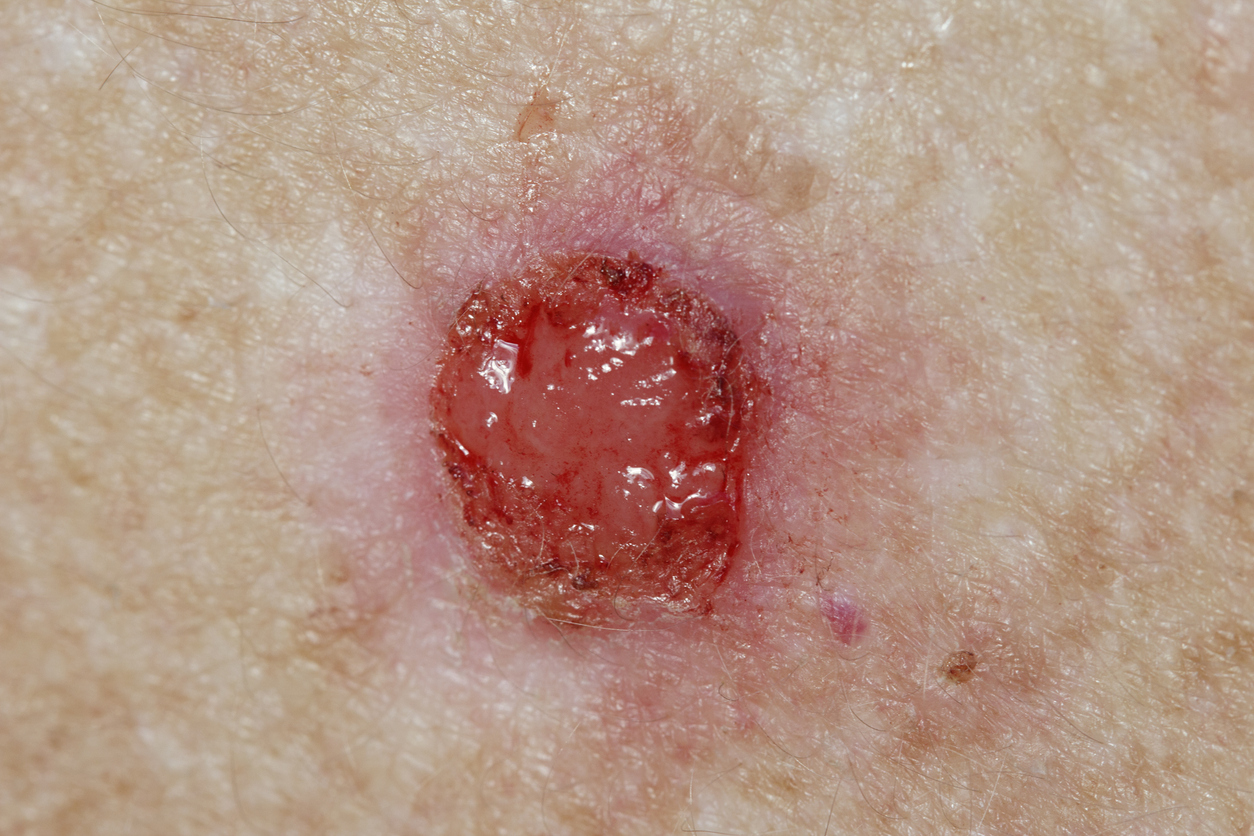
BCC doesn’t always look dramatic. Many people assume it’s a “stubborn spot” until it keeps hanging around. Common appearances include:
A simple rule that helps: if a spot lasts more than 4–6 weeks, keeps coming back, or is slowly changing, it’s worth getting checked—especially if it’s on the face.
BCC often causes no pain, which is why it can be ignored for longer than it should be. But it may:
Symptoms can come and go, and some people feel nothing at all. That’s why the behaviour of the lesion (not healing, recurring bleeding, slowly enlarging) is often more helpful than how it feels.
Yes—mainly because of what it can do locally. While BCC very rarely spreads to other organs, it can still become more complicated if it’s left untreated. Over time it may:
In high-visibility or delicate areas—like the nose, eyelids, lips, ears, and temples—earlier treatment usually means a smaller procedure and less disruption to the shape and function of the area.
Diagnosis usually begins with a clinical assessment. A clinician will examine the area closely and may use a dermatoscope (a handheld magnifier with light) to look at skin patterns that are not visible to the naked eye.
If BCC is suspected, the next step is typically a skin biopsy. This involves numbing the area and removing a small sample of skin (or sometimes the whole lesion, depending on size and location). The sample is then examined under a microscope to confirm:
The biopsy is usually quick, and most people tolerate it very well.
Treatment is tailored to the individual lesion and to you. The “best” approach depends on:
Common treatment options include:
Surgical removal (excision)
This involves removing the BCC along with a margin of surrounding skin, then closing the area with stitches. The removed tissue is checked in a lab to confirm it has been fully removed.
Mohs surgery (selected cases)
Mohs is often recommended for certain BCCs, particularly on the face, in areas where we want to preserve as much normal tissue as possible, or when the lesion has returned. (Since you have a separate Mohs page, the key point here is simply that it is a highly precise option used in specific situations.)
Curettage and cautery / electrosurgery (selected cases)
For some smaller, lower-risk BCCs in suitable locations, the lesion may be scraped and treated to destroy remaining abnormal cells. This can be effective in the right setting but isn’t ideal for every subtype or every area.
Topical treatments (selected cases)
Some superficial BCCs can be treated with prescription creams. These are not suitable for deeper or more aggressive subtypes, and they generally require consistent application and follow-up.
Radiotherapy (selected cases)
Radiation can be used in some situations—especially when surgery is not ideal—though it often involves multiple visits and isn’t the first choice for everyone.
Your clinician will discuss why a specific approach is recommended in your case, what the cure rates are, what kind of scarring to expect, and what recovery will look like.
Most people do really well after BCC treatment, and in many cases the cancer is completely removed with no further issues at that site. Long-term care is mainly about three things: (1) healing well, (2) monitoring for recurrence, and (3) reducing the chance of developing a new skin cancer elsewhere.
It’s normal for the treated area to look and feel “different” for a while. Scars don’t settle instantly—skin healing is a slow, staged process.
A few sensations can be normal during scar maturation:
If your scar becomes increasingly painful, hot, or rapidly more swollen, that’s not typical and should be checked.
After a BCC is treated, there is still a small chance it can come back in the same area, especially if it had higher-risk features (for example, a previous recurrence, an ill-defined border, or certain subtypes).
What recurrence might look like:
Recurrences are often easier to manage when found early—so it’s worth checking anything suspicious rather than waiting it out.
This is the part that surprises many people: even if your treated BCC is gone for good, having had one BCC means your skin has had enough UV damage to develop a skin cancer—so the risk of another BCC (or another type of skin cancer) is higher over time.
This doesn’t mean something will definitely come back. It just means that long-term monitoring and sun protection are genuinely worthwhile because they reduce future risk and help you catch changes early.
Follow-up plans vary depending on your personal risk factors (how many lesions you’ve had, where it was, what type it was, your age, immune status, and sun exposure history). In general, follow-up may include:
If you’ve had multiple BCCs, your clinician may recommend more regular checks.
Self-checks don’t need to be intense or anxious—they’re just a habit.
A good rhythm is:
What to look for:
Taking a quick phone photo every few weeks can help you notice slow changes that are easy to miss day-to-day.
Sun protection isn’t about never going outside—it’s about lowering your lifetime UV exposure from here.
Practical habits that work:
If your treated area is still healing, sun protection matters even more—new scar tissue can pigment more easily and may stay red longer if it’s exposed to UV.
You should reach out if you notice:
ACC funding eligibility is determined by the Accident Compensation Corporation on a case-by-case basis. Approval is dependent on injury acceptance, clinical indication, and ACC policy at the time of application. Not all treatments offered at Scars & Lasers are ACC-funded. Private fees may apply for unfunded components of care.


